1.07 High blood pressure
Page content
Why is it important?
High blood pressure, also referred to as hypertension, is a major risk factor for stroke, coronary heart disease, heart failure, kidney disease, deteriorating vision and peripheral vascular disease leading to leg ulcers and gangrene. High blood pressure is defined as a systolic blood pressure greater than 140 mmHg and/or diastolic pressure greater than 90 mmHg and/or patient receiving medication for high blood pressure (NHF, 2016). Major risk factors for high blood pressure include increasing age, poor diet (particularly high salt intake), obesity, excessive alcohol consumption, and insufficient physical activity (WHO, 2013; AIHW, 2015b) . A number of these risk factors are more prevalent among Indigenous Australians (see measures in Health Behaviours).
A study of Indigenous Australians living in urban WA found that, after controlling for other cardiovascular risk factors, those with high blood pressure were twice as likely to die or be hospitalised due to a cardiovascular event (Bradshaw et al, 2009).
While for some people, the propensity to develop high blood pressure appears to be inherited, it can often be prevented or controlled by leading an active and healthy life, remaining fit, avoiding obesity, albuminuria and diabetes and, if necessary, taking regular medication (Semlitsch et al, 2013; Bunker, 2014; Li, M & McDermott, 2015; NHF, 2016). For those with high blood pressure, treatment with long-term medication can reduce the risk of developing complications, although not necessarily to the levels of unaffected people (AIHW, 2015a). Reducing the prevalence of high blood pressure is one of the most important means of reducing serious circulatory diseases, which are the leading cause of death among Indigenous Australians (see measure 1.23).
Findings
High blood pressure was responsible for 5% of the Indigenous burden of disease and 8% of the health gap between Indigenous and non-Indigenous Australians in 2011 (AIHW, 2016f). High blood pressure contributed to 64% of the burden due to hypertensive heart disease, 61% of the stroke burden, and 37% of the coronary heart disease burden. Most high blood pressure burden for Indigenous Australians was due to early death (88%), predominantly in the 45–69 year age group and higher for males (60%) than females (40%).Between 2003 and 2011 there was a 23% reduction in burden of disease attributable to high blood pressure for Indigenous Australians.
Based on both measured and self-reported data from the 2012–13 Health Survey, 27% of Indigenous adults had high blood pressure. Rates increased with age and were higher in remote areas (34%) than non-remote areas (25%). Twenty per cent of Indigenous adults were found to have high blood pressure during the survey interview. Of these adults, 21% also reported diagnosed high blood pressure. Most Indigenous Australians with measured high blood pressure in the survey (79%) had not previously been diagnosed with the condition; this proportion was similar among non-Indigenous Australians. Therefore, there are a number of Indigenous adults with undiagnosed high blood pressure who are unlikely to be receiving appropriate medical advice and treatment. The proportion of Indigenous adults with measured high blood pressure who did not report a diagnosed condition decreased with age and was higher in non-remote areas (85%) compared with remote areas (65%). In 2012–13, 10% of Indigenous adults reported they had a diagnosed high blood pressure condition. Of these, 18% did not have measured high blood pressure and therefore are likely to be managing their condition. Indigenous males were more likely to have high measured blood pressure (23%) than females (18%). The survey showed that an additional 36% of Indigenous adults had pre-hypertension (blood pressure between 120/80 and 140/90 mmHg). This condition is a signal of possibly developing hypertension requiring early intervention.
In 2012–13, after adjusting for differences in the age structure of the two populations, Indigenous adults were 1.2 times as likely as non-Indigenous adults to have measured high blood pressure. For Indigenous Australians, rates started rising at younger ages and the largest gap was in the 35–44 year age group. The 2012–13 Health Survey showed a number of associations between socio-economic status and measured and/or self-reported high blood pressure. Indigenous Australians living in the most relatively disadvantaged areas were 1.3 times as likely to have high blood pressure (28%) as those living in the most relatively advantaged areas (22%).
Indigenous Australians reporting having completed schooling to Year 9 or below were 2.1 times as likely to have high blood pressure (38%) as those who completed Year 12 (18%). Additionally, those who were obese were 2 times as likely as those not obese to have high blood pressure (37% vs 18%). Those reporting fair/poor health were 1.8 times as likely as those reporting excellent/very good/good health to be have high blood pressure (41% vs 22%). Those reporting having diabetes were 2.2 times as likely to have high blood pressure (51% vs 23%), as were those reporting having kidney disease (57% vs 26%).
One study in selected remote communities found high blood pressure rates 3–8 times those in the general population (Hoy, WE et al, 2007). A long-term follow-up study in rural and remote communities in Northern Australia found the incidence of hypertension in Indigenous adults was nearly double the non-Indigenous rate. Increased incidence of obesity, diabetes and albuminuria were found to contribute to this higher rate (Li, M & McDermott, 2015).
Most diagnosed cases of high blood pressure are managed by GPs or medical specialists. When hospitalisation occurs it is usually due to cardiovascular complications resulting from uncontrolled chronic blood pressure elevation. During the two years to June 2015, hospitalisation rates for hypertensive disease were 2.3 times as high for Aboriginal and Torres Strait Islander peoples as for non-Indigenous Australians. Among Aboriginal and Torres Strait Islander peoples, hospitalisation rates started rising at younger ages with the greatest difference in the 55–64 year age group. This suggests that high blood pressure is more severe, occurs earlier, and is not controlled as well for Indigenous Australians. As a consequence, severe disease requiring acute care in hospital is more common.
Based on GP survey data (2010–15), high blood pressure represented nearly 4% of all problems managed by GPs among Indigenous patients. Rates were similar for both Indigenous and other Australian patients (after adjusting for differences in the age structure of the two populations).
In May 2015, Commonwealth-funded Indigenous primary health care organisations provided national Key Performance Indicators data based on best practice guidelines. Of the 32,900 regular clients with Type 2 diabetes, 68% had their blood pressure assessed and 43% had results in the recommended range in the six months to May 2015.
Figures
Figure 1.07-1
Aboriginal and Torres Strait Islander people with measured/self-reported high blood pressure by age and remoteness, 2012–13
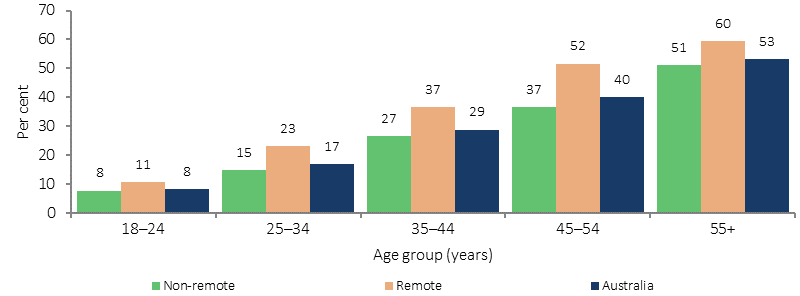
Source: ABS and AIHW analysis of 2012–13 AATSIHS
Figure 1.07-2
Proportion of Aboriginal and Torres Strait Islander people 18 years and over by blood pressure group and whether blood pressure was self-reported, 2012–13
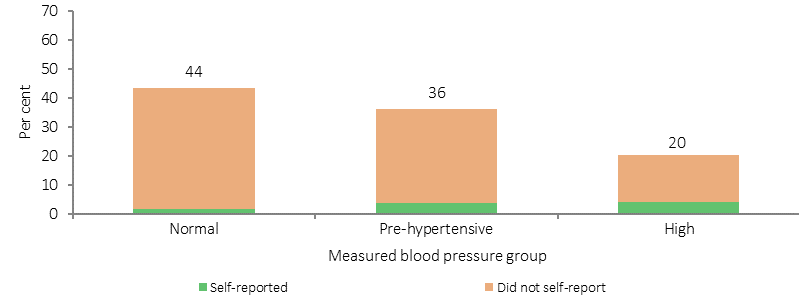
Source: ABS and AIHW analysis of 2012–13 AATSIHS
Figure 1.07-3
Measured high blood pressure, by Indigenous status, age and sex, 2011–13
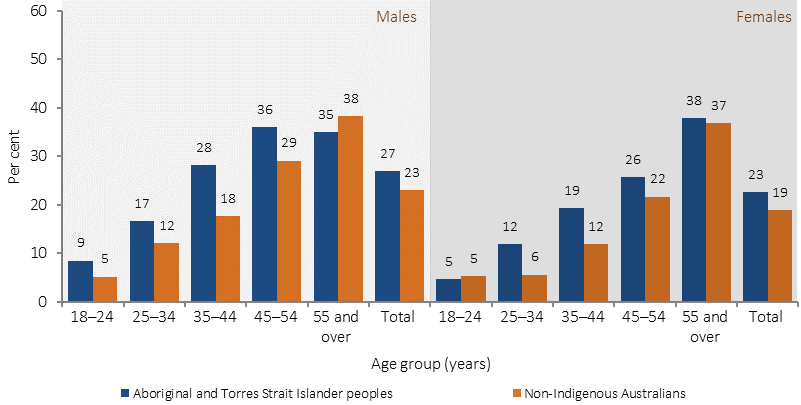
Note: Total is age-standardised.
Source: ABS and AIHW analysis of 2012–13 AATSIHS
Implications
The prevalence of measured high blood pressure among Indigenous adults was estimated as 1.2 times as high as for non-Indigenous adults and hospitalisation rates were 2.3 times as high, but high blood pressure accounted for a similar proportion of GP consultations for both populations. This suggests that Indigenous Australians are less likely to have their high blood pressure diagnosed and less likely to have it well controlled given the similar rate of GP visits and higher rate of hospitalisations due to cardiovascular complications.
Identification and management of hypertension requires access to primary health care with appropriate systems for the identification of Aboriginal and Torres Strait Islander clients and systemic approaches to health assessments and chronic illness management. Research into the effectiveness of quality improvement programmes in Aboriginal and Torres Strait Islander primary health care services has demonstrated that blood pressure control and hence CVD prevention can be improved by a well-coordinated and systematic approach to chronic disease management (McDermott et al, 2003; Burgess, CP et al, 2015).
The Indigenous Australians' Health Programme (IAHP) focuses on the prevention, early detection, and management of chronic disease, including high blood pressure, through expanded access to and coordination of comprehensive primary health care. Activities funded under the IAHP include Tackling Indigenous Smoking; a care coordination and outreach workforce based in AMSs and mainstream services; and GP, specialist and allied health outreach services serving urban, rural and remote communities.
In addition to the activities funded under the IAHP, the Australian Government provides funding for GP health assessments for Aboriginal and Torres Strait Islander people under the MBS, which includes blood pressure measurement and follow-on care. Funding is also provided for incentive payments for improved health care management, and for cheaper medicines through the PBS.