2.21 Health behaviours during pregnancy
Page content
Why is it important?
Many lifestyle factors contribute to, and can have adverse effects on, the health and wellbeing of a woman and her baby during pregnancy and birth, as well as outcomes for children later in life.
Tobacco smoking increases the risk of pregnancy complications (e.g. miscarriage, placental abruption and premature labour); and poor perinatal outcomes such as low birthweight, intrauterine growth restriction, pre-term birth and perinatal death (Pringle et al, 2015; Hodyl et al, 2014; Wills & Coory, 2008; Laws & Sullivan, 2005; England et al, 2004). Maternal exposure to second hand smoke also increases these risks for babies (Crane et al, 2011) (see measure 2.03 for effects of second hand smoke exposure after birth). There is evidence that smoking cessation, particularly in the first trimester, can reduce these risks (Yan & Groothuis, 2015; Hodyl et al, 2014; Bickerstaff et al, 2012).
Drinking alcohol while pregnant may result in miscarriage, stillbirth, low birthweight, intrauterine growth restriction and prematurity and has been shown to result in a range of potentially lifelong physical, mental, behavioural and/or learning issues, collectively referred to as Foetal Alcohol Spectrum Disorders (FASD) (Mutch et al, 2015; Srikartika & O'Leary, 2015; France et al, 2010). Nationally, the true prevalence of FASD for Indigenous Australians is not known; estimates vary from 2.7 to 4.7 per 1,000 births (House of Representatives, 2012). A recent study in Fitzroy Valley found rates to be 120 per 1,000 children (Fitzpatrick et al, 2015). While existing research has limitations, risks of harm are said to increase with the amount and frequency of alcohol consumed (O'Leary et al, 2010). The NHMRC recommends not drinking alcohol during pregnancy as the safest option (NHMRC, 2009).
Use of illicit drugs (e.g. heroin, cannabis) and some licit drugs (e.g. medicines) during pregnancy can pose health risks to the mother (e.g. overdose and accidental injuries) as well as significant obstetric, foetal and neonatal complications (Kennare et al, 2005; Kulaga et al, 2009; Ludlow et al, 2004; Wallace, C et al, 2007) and behavioural and cognitive problems that emerge in later life (Passey et al, 2014).
Nutrition before and during pregnancy is also critical to foetal development (McDermott et al, 2009; Wen et al, 2010). Pregnant women and women considering pregnancy are advised to have a balanced diet. Maintenance of folate levels are particularly important to decrease risk of neural tube defects such as spina bifida (AHMAC, 2012), which is twice as common among babies born to Indigenous women as those born to non-Indigenous women (AIHW NPSU, 2011). In addition to adverse birth outcomes, poor maternal nutrition has been linked with increased risk of developing insulin resistance and obesity in their children (Drake & Reynolds, 2010; Nelson, SM et al, 2010).
Findings
According to 2014 perinatal data, 46% of Aboriginal and Torres Strait Islander mothers smoked during pregnancy. Nationally (excluding Vic), between 2006 and 2014 the smoking rates among Indigenous mothers declined by 13% (from 54% to 46% respectively). After adjusting for the different age structures of the two populations, Indigenous mothers were 3.6 times as likely to smoke during pregnancy as non-Indigenous mothers. In 2014, Indigenous mothers were half as likely to stop smoking during pregnancy as non-Indigenous mothers (12% compared with 24%).
Further to this, 2014 perinatal data showed no clear pattern of smoking by age group for Indigenous mothers (and teenage mothers were not the group with the highest rate). For non-Indigenous mothers, those under 20 years of age had the highest rate of smoking (30%), followed by 20–24 year olds (20%) and was between 6% and 10% for the age groups 25 years and over.For Indigenous mothers smoking rates were lower in major cities (41%) compared with 51% in very remote areas.
A multivariate analysis of 2012–14 perinatal data indicates that, excluding pre-term and multiple births, 51% of low birthweight babies born to Indigenous mothers were attributable to smoking during pregnancy, compared with 16% for other mothers. After adjusting for age differences and other factors, it was estimated that if the Indigenous maternal smoking rate was the same as that of other mothers, the proportion of low birthweight babies could be reduced by 40% (see measure 1.01). Babies born to Indigenous mothers who smoked were 1.5 times as likely to be pre-term as those who did not smoke.
Studies have found that smoking during pregnancy among Indigenous women is associated with low socio-economic status; stress; social norms, including number of smokers in the household; and lack of knowledge regarding consequences of smoking during pregnancy, which in turn influence incentives and support to quit (Johnston et al, 2011; Wood et al, 2008; Passey et al, 2012; Thrift et al, 2011). Social Survey data from 2014–15 showed that 39% of Indigenous mothers of children aged 0–3 years smoked during pregnancy. This rate is lower than the rate from perinatal data, however it should be noted that the survey data is self-reported and subject to sample error.
Based on self-reported data for Indigenous mothers of children aged 0–3 years (2014–15 Social Survey), the vast majority reported that they did not consume alcohol (91%) or use illicit drugs (96%) during pregnancy. In 2014–15, the proportion of Indigenous children aged 0–3 years who had a birth mother who drank alcohol during pregnancy halved from 20% in 2008 to 10% in 2014–15, with the largest decline in non-remote areas (10 percentage points). On average, 60% of Indigenous mothers took folate before or during pregnancy, dropping to 33% in very remote areas.
According to 2014 perinatal data, Indigenous mothers were 1.7 times as likely to be obese, 3 times as likely to have pre-existing diabetes and more than twice as likely to have pre-existing hypertension than non-Indigenous mothers.
A study of 476 Aboriginal and Torres Strait Islander women attending 34 Indigenous community health centres across Australia found that 46% of those who smoked received documented advice about smoking cessation (Rumbold et al, 2011). Only 27% of women in this study were prescribed folic acid prior to 20 weeks gestation and even fewer (8%) prior to conception. These findings may be influenced by later presentation for antenatal care (see measure 3.01) (Robinson, P et al, 2012).
Figures
Figure 2.21-1
Age-standardised proportion of mothers who smoked during pregnancy, by Indigenous status and remoteness, 2014
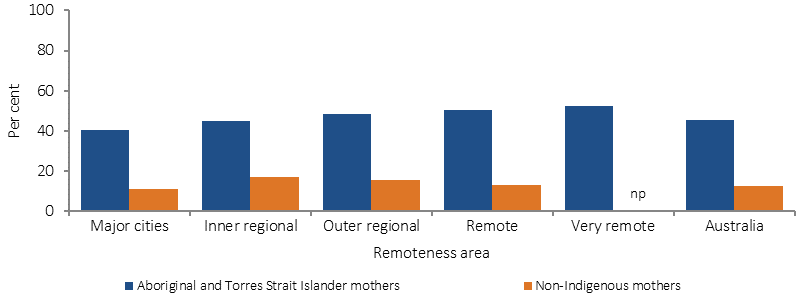
Source: AIHW analysis of the 2014 National Perinatal Data Collection.
Figure 2.21-2
Proportion of mothers who smoked during pregnancy, by Indigenous status and age of mother, 2014
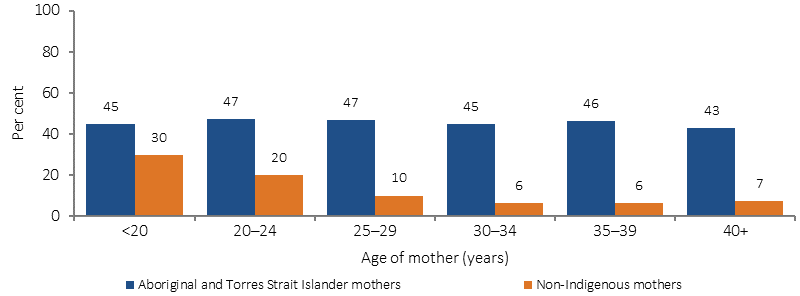
Source: AIHW analysis of the 2014 National Perinatal Data Collection
Figure 2.21-3
Age-standardised percentage of mothers who smoked during pregnancy by Indigenous status, 2006 to 2014
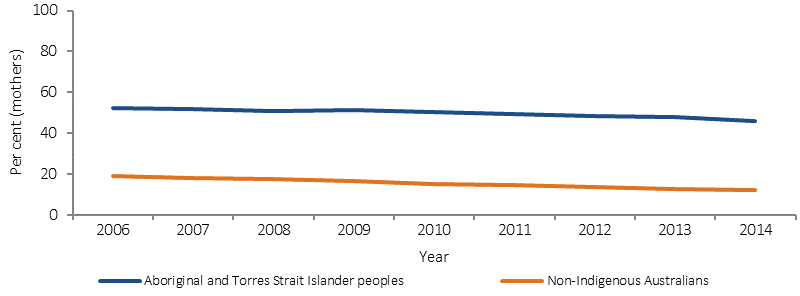
Source: AIHW/NPESU analysis of 2014 National Perinatal Data Collection
Figure 2.21-4
Use of tobacco, alcohol and illicit drugs during pregnancy, mothers of Indigenous children (0–3 years), 20 14–15
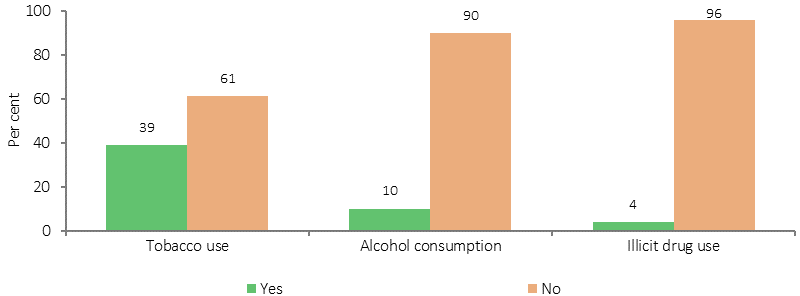
Source: ABS and AIHW analyses of 2014–15 NATSISS
Implications
Expanding national data on health behaviours during pregnancy will be an important element of monitoring progress in this area.
There is little evidence on cessation or education strategies that work (Eades, S et al, 2012; Hefler & Thomas, 2013; Lucas et al, 2014; Bower et al, 2004). Recommended approaches are those that: consider social and environmental contexts; increase knowledge of harm and cessation methods; are tailored to clients’ needs; are provided in a way that does not cause embarrassment or distress or deter further antenatal care; are culturally targeted with Indigenous health worker involvement; include partners, families and communities; are provided before, during and after pregnancy; and include alternative stress reduction and coping strategies (Bond et al, 2012; Gould et al, 2013; van der Sterren & Fowlie, 2015; France et al, 2010; Bridge, 2011; Elliott & Silverman, 2013; Wood et al, 2008; Marley et al, 2014)
Concurrent use of multiple substances and clustering of risk factors, particularly for women of lower socio-economic status, also need to be considered and addressed through holistic approaches (Passey et al, 2014; Wen et al, 2010; Eades, S et al, 2012; Brown, SJ et al, 2016a).
The 2014–15 Budget provided funding of $94 million over three years from July 2015, for the Better Start to Life approach to expand efforts in child and maternal health. This included expanding New Directions: Mothers and Babies Services and the Australian Nurse Family Partnership Program (ANFPP). As part of the Women’s Safety Package, the Australian Government has also committed $1.1 million to enhance the ability of the ANFPP to support families who might be experiencing domestic violence.
The Indigenous Australians’ Health Programme includes $12 million over two years (from July 2016) to support the implementation of integrated early childhood services: Connected Beginnings, as recommended by the Forrest Review. The Department of Education has also allocated $30 million over three years to support the program.
National Evidence-Based Antenatal Care Guidelines have been developed, with advice specific to meeting the needs of Aboriginal and Torres Strait Islander pregnant women and advice on health behaviours during pregnancy.
The National Tobacco Campaign, Quit for You, Quit for Two is aimed at reducing smoking prevalence among pregnant women, their partners and women who are contemplating pregnancy. Materials feature Indigenous women (see 2.15). In Tasmania, the Smoke Free Pregnancies Working Group has implemented A Smoke Free Start for Every Tasmanian Baby: A Plan for Action—2014 to 2017. The Aboriginal and Torres Strait Islander Smoking Cessation Program supports a number of smoking cessation activities in the ACT, with an emphasis on pregnant smokers and their cohabitants.
Under the Tackling Indigenous Smoking (TIS) program (see measure 2.15), regional grants allow for focused work on priority groups such as pregnant women and relationships with other programs for mothers and babies. Grants for three projects specifically targeting pregnant women have been awarded under the TIS innovation grant scheme.
In the 2014–15 Budget, the National Foetal Alcohol Spectrum Disorders (FASD) Action Plan was allocated $9.2 million, with an additional $10.5 million over four years allocated in 2016–17. Various activities are being undertaken across jurisdictions. For example, in WA, the FASD Prevention Program in the Kimberly region, run by the Ord Valley Aboriginal Health Service, provides education and support of antenatal clients and their families, as well as education sessions to students in the region.
The Pregnancy, Birth and Baby helpline and website, provides a range of support to women, partners and families in relation to pregnancy and parenting.
See the Policies and Strategies section for full details.