3.09 Discharge against medical advice
Page content
Why is it important?
Indigenous Australians are more likely than non-Indigenous Australians to leave hospitals without completing treatment. Patient experiences of health care services impact on health-related behaviours and health outcomes. People who take their own leave from hospital are more likely to re-present to emergency departments and have higher mortality rates (Shaw, 2016).
The measure reported here is based on the extent to which Aboriginal and Torres Strait Islander people ‘vote with their feet’ (i.e. in discharging themselves from hospital against medical advice). The measure provides indirect evidence of the extent to which hospital services are responsive to Indigenous Australian patients’ needs. There have been a limited number of studies on the reasons Indigenous Australians take their own leave from hospital. However common factors include: institutionalised racism; a lack of cultural safety; a distrust of the health system; miscommunication; family and social obligations; isolation and loneliness; a lack of understanding of the treatment they were receiving and feeling that the treatment had finished; and communication and language barriers between staff and patient (Shaw, 2016).
Findings
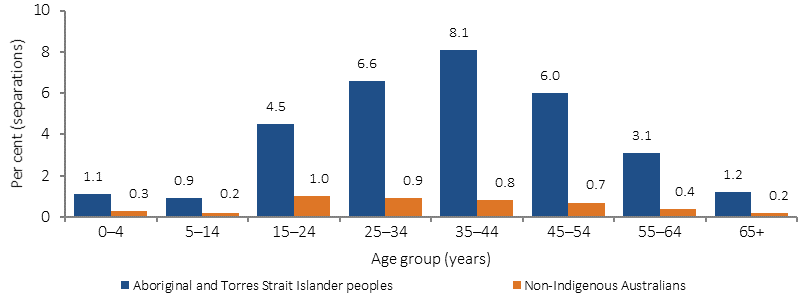
Between July 2013 and June 2015, there were 18,427 hospitalisations where Aboriginal and Torres Strait Islander people left hospital against medical advice or were discharged at their own risk. After adjusting for age, this represented 3.4% of all hospitalisations for Aboriginal and Torres Strait Islander peoples compared with 0.5% for non-Indigenous Australians. Indigenous Australians were discharged from hospital against medical advice at 7 times the rate of non-Indigenous Australians.
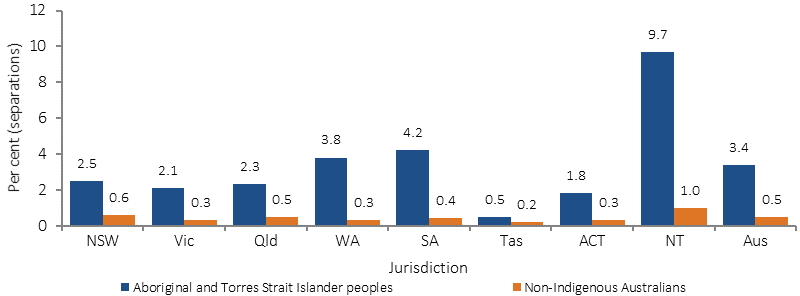
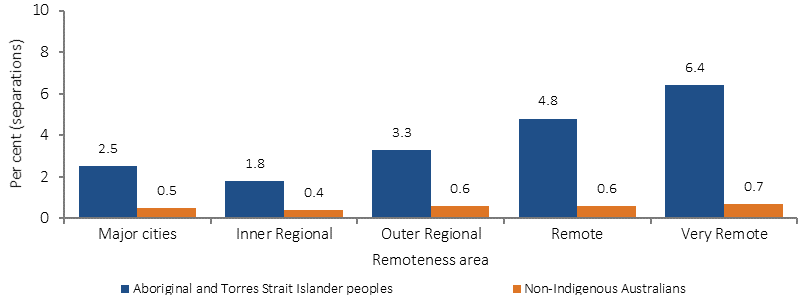
Discharges from hospital against medical advice are most common for Aboriginal and Torres Strait Islander peoples aged 25–54 years. They are also more common for Indigenous Australians living in remote and very remote areas. The proportion of discharge against medical advice for Aboriginal and Torres Strait Islander peoples was highest in the NT (10% of all hospitalisations) and lowest in Tasmania, and the ACT (both less than 2%).
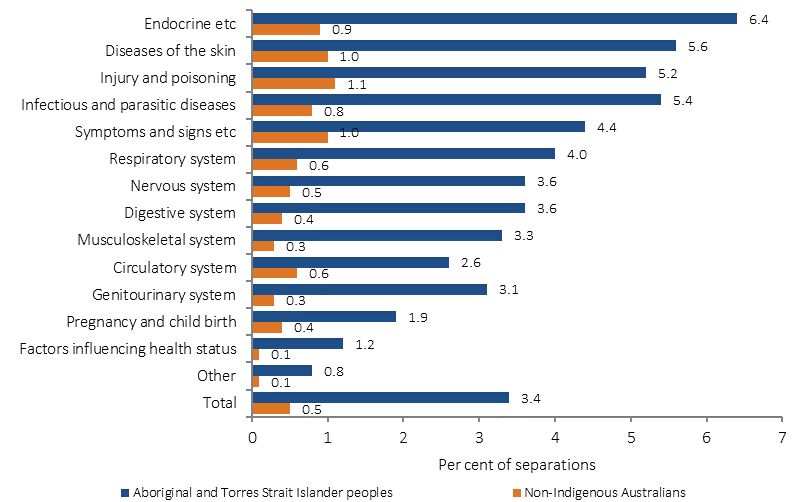
Among Indigenous Australians who were discharged against medical advice, the most common principal diagnoses for hospitalisations were injury and poisoning (4,019 hospitalisations), followed by symptoms, signs and abnormal clinical and laboratory findings not elsewhere classified (2,322 hospitalisations) and respiratory disease (2,098 hospitalisations). These three groups of diagnoses represented 46% of all hospitalisations for which Indigenous patients were discharged against medical advice. As a proportion of all hospitalisations of Indigenous Australians for each specific diagnoses group, discharge against medical advice was highest for endocrine, nutritional and metabolic disorders (including diabetes) (7.4%), followed by injury and poisoning and external causes (7.0%).
An analysis of the relative impact of a range of factors over the period July 2013 to June 2015 found that Indigenous status was the single most significant variable contributing to whether a patient would discharge themselves from hospital against medical advice, even after controlling for the other factors. Other factors that were significant in order of importance after Indigenous status were:
- sex
- principal diagnosis
- age group
- remoteness of hospital
- state/territory of hospital
- remoteness of usual residence
- state/territory of usual residence.
In 2015–16, there were around 12,000 Emergency Department presentations for Indigenous Australians where the patient left at own risk. After adjusting for age, Indigenous patients were more likely than non-Indigenous patients to leave at their own risk (2.3% of presentations compared with 1.7%). There were around 27,000 Emergency Department presentations for Indigenous Australians where the patient did not wait. Indigenous patients were more likely than non-Indigenous patients to not wait (5.2% of presentations compared with 3.5%).
Figures
Figure 3.09-1
Proportion of hospitalisations ending in discharge against medical advice, by Indigenous status and age group, July 2013–June 2015
Source: AIHW National Hospital Morbidity Database
Figure 3.09-2
Proportion of hospitalisations ending in discharge against medical advice, by Indigenous status and jurisdiction, July 2013–June 2015
Source: AIHW National Hospital Morbidity Database
Figure 3.09-3
Proportion of hospitalisations ending in discharge against medical advice, by Indigenous status and remoteness, July 2013–June 2015
Source: AIHW National Hospital Morbidity Database
Figure 3.09-4
Proportion of hospitalisations ending in discharge against medical advice, by Indigenous status and principal diagnosis, July 2013–June 2015
Source: AIHW National Hospital Morbidity Database
Implications
The elevated levels of discharge against medical advice suggest that there are significant issues in the responsiveness of hospitals to the needs and perceptions of Aboriginal and Torres Strait Islander peoples (see measure 3.08). Mechanisms for obtaining feedback from Aboriginal and Torres Strait Islander patients will assist in responding and planning in relation to these rates of discharge against medical advice. The data suggest these issues are important for all age groups, although the issues are most evident for those aged 25–54 years.
There are several questions for health service researchers and health service managers to tackle in devising strategies to achieve more responsive and respectful service delivery. More needs to be known about the reasons for the high rates of discharge against medical advice across individual factors (such as personal circumstances, health and wellbeing, and cultural issues); community level factors (such as levels of trust or mistrust in the health system); and hospital level factors (such as staff attitudes, hospital policies and the environment). Historical issues, such as segregation and hospitals being seen as a place to go to die are also factors to be investigated. Hospitals and health services that have implemented successful programs to reduce discharge against medical advice need to be studied and lessons disseminated.
AHMAC has funded work to develop a national framework to address key contributing and protective factors to reduce the rates of Aboriginal and Torres Strait Islander people ‘taking their own leave’ and ‘discharging against medical advice’ from Australian hospitals. This includes addressing factors that impact on access to hospital services by Aboriginal and Torres Strait Islander people, developing consumer-centred approaches that improve the health journey and the hospital environment, and improving the capability of hospitals to deliver culturally appropriate care for Aboriginal and Torres Strait Islander people.
The Australian Government through the Implementation Plan for the National Aboriginal and Torres Strait Islander Health Plan 2013–2023, has committed to reducing discrimination in the health system and improve the accessibility of health services for Aboriginal and Torres Strait Islander people. This includes funding for projects that improve Indigenous patient outcomes, such as the Lighthouse Hospital Project, which aims to drive systemic change in the acute care sector to improve care and outcomes for Aboriginal and Torres Strait Islander people who experience acute coronary syndrome.