3.22 Recruitment and retention of staff
Page content
Why is it important?
The capacity to recruit and retain appropriate staff is critical to the appropriateness, continuity and sustainability of health services including Aboriginal and Torres Strait Islander primary health care services. Staff recruitment and retention is particularly important in rural and remote areas as 65% of Indigenous Australians live outside the major cities.
Findings
In 2015, there were 97,466 medical practitioners registered in Australia (excluding provisional registrants), with 86% employed as clinicians. Many of those not working in medicine were overseas, retired or on extended leave. The supply of practitioners working as clinicians increased between 2005 and 2015 (from 298 to 375 FTE per 100,000 population). Supply was not uniform across the country; it was greater in major cities (421 FTE per 100,000) than in remote/very remote areas (251 FTE per 100,000). While GP rates per 100,000 were similar across geographic areas, the supply of specialists was much lower in remote/very remote areas (AIHW, 2016g). Rural outreach is provided by specialists who periodically visit the same community over time. In a 2014 study, 19% of specialist doctors provided outreach. Three-quarters of these were metropolitan-based (O’Sullivan et al, 2014).
A national survey of the rural workforce in November 2015 found that of the 7,841 GPs working in rural Australia, an estimated 48% had been in their current practice for less than 3 years (56% in remote and very remote areas). A 2015 study on GP mobility found that GPs working in small communities and those in rural locations for less than 3 years are most at risk of leaving rural practice (McGrail & Humphreys, 2015). Younger rural GPs were also more likely to leave rural practice than older rural GPs.
A 2007 study identified doctors who were satisfied with their current medical practice intended to remain in rural practice for 40% longer than those who were not satisfied (11.5 years compared with 8.2 years). GPs content with their life as a rural doctor intended to remain in rural practice 51% longer than those who were not content (11.8 compared with 7.8 years) (Alexander & Fraser, 2007).
For other health professions, National Health Workforce Data indicate that 85% of trained nurses were currently working in the nursing sector in 2015 (AIHW, 2016d). In 2014, 89% of dental practitioners were employed in dentistry. For other health professionals, the proportions working in their field were as follows: physiotherapists (83%), pharmacists (85%), psychologists (86%), Aboriginal and Torres Strait Islander health practitioners (83%), optometrists (89%), chiropractors (88%), osteopaths (89%), and podiatrists (92%).
In 2014, the number of employed psychologists was lowest in areas with high proportions of Indigenous Australians in the population (44 per 100,000 in areas with 20% or more Indigenous Australians in the population compared with 115 per 100,000 in areas with less than 1%). The pattern was similar for pharmacists.
As at 31 May 2015, there were around 4,700 FTE health (clinical) staff and 2,900 FTE administrative and support staff positions within Commonwealth-funded Indigenous primary health care (PHC) organisations. In the period 1999–2000 to 2014–15, there was an increase of 331% in the number of FTE staff in these organisations. Despite this growth, the vacancy rate has improved with an estimated 5% of health positions and 1% of administrative and support staff positions vacant at 31 May 2015, compared with 7% and 3% at June 2000.
Vacancies in Commonwealth-funded Indigenous PHC organisations were highest for Aboriginal Health Workers (64 vacant FTEs) followed by nurses (34 FTE), social and emotional wellbeing workers (25 FTE) and Aboriginal Health Practitioners (23 FTE) in 2015. The proportion of health staff positions that were vacant ranged from 8% in very remote areas to 3% in major cities. For administrative/support positions, vacancies were also highest in very remote areas (3%) while less than 2% elsewhere (AIHW, 2016o).
In 2014–15, 66% of Commonwealth funded Indigenous organisations reported the recruitment, training and support of Aboriginal and Torres Strait Islander staff as one of the top five challenges in providing quality care to clients. In remote areas, this was as high as 85%. Among all staff, retention and turnover was reported as a challenge by 54% of organisations—highest in remote (58%) and very remote areas (67%) where staff housing was also a challenge (54% and 51% respectively compared with 28% overall) (AIHW, 2016o).
A senate inquiry into factors affecting the supply of health services and medical professionals in rural areas (SCACS, 2012) has identified a complex interplay between environmental, personal and work-related factors. These include access to professional development and career progression; remuneration; heavy workloads; on-call hours; loss of anonymity; social barriers and professional isolation; opportunities for spouses and children; and access to appropriate, affordable and secure accommodation. A growing trend towards medical specialisation was identified as reducing generalist training pathways—the area of medical practice most required in rural and regional areas. Conversely rural lifestyle, diverse caseloads, autonomy and community connectedness have been cited as positive influences (Campbell, N et al, 2012).
A study of drug and alcohol workers found that Indigenous workers experienced above average levels of job satisfaction and relatively low levels of exhaustion; however, they also experienced lower levels of mental health and wellbeing and greater work/family imbalance. The report highlighted the importance of workforce development strategies that focus on culturally appropriate, equitable and supportable organisational conditions including addressing stress, salaries, benefits and opportunities for career and personal growth (Roche et al, 2013).
Figures
Figure 3.22-1
Employed medical practitioners: FTE per 100,000 population by remoteness area and main field of medicine, 2015
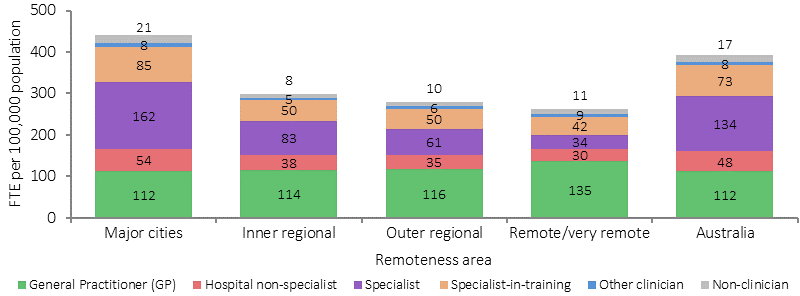
Source: National Health Workforce Data Set: Medical Practitioners 2015 (AIHW, 2015)
Figure 3.22-2
Proportion of GPs in rural and remote areas, by length of stay in current practice, 30 November 2015
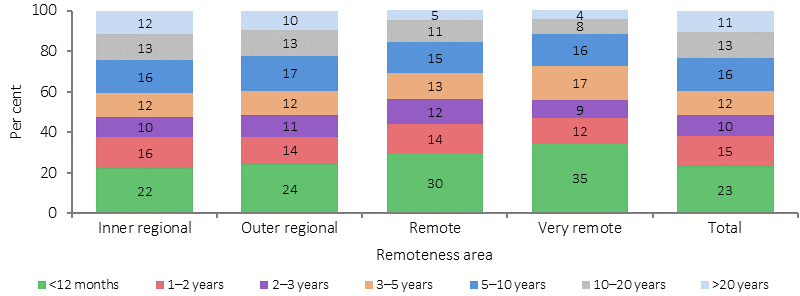
Source: AIHW analysis of Rural Workforce Agencies NMDS
Figure 3.22-3
Vacant FTE positions as a proportion of total funded positions, by position type and remoteness area, Indigenous primary health care organisations, as at 31 May 2015
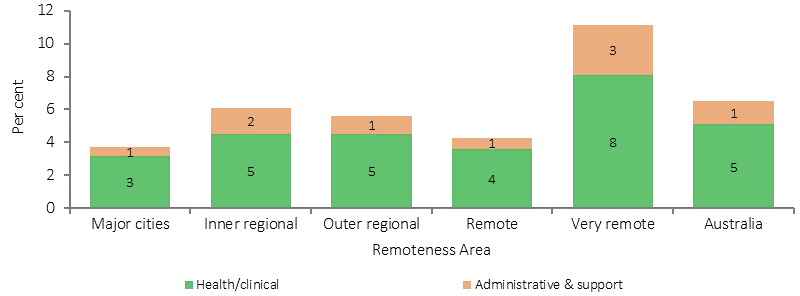
Source: AIHW 2016
Figure 3.22-4
Vacant FTE positions as a proportion of total funded positions, by position type, Indigenous primary health care organisations, 30 June 2000 to 31 May 2015
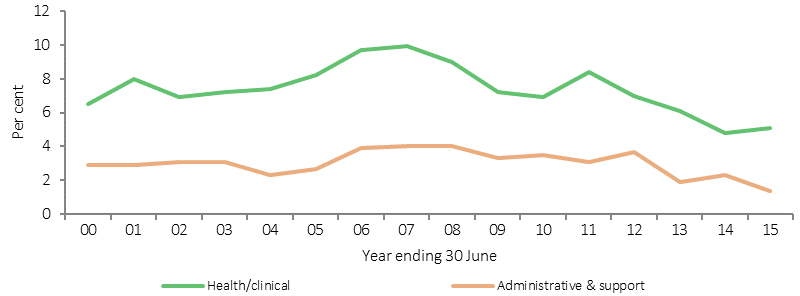
Source: AIHW analyses of SAR, DSR and OSR data collections
Implications
Better national data are needed on this important issue. The statistics analysed focus on a few aspects of a complex set of issues. Recruitment and retention issues are significant for health services located in rural and remote Australia. Little is known about the turnover of staff in Indigenous primary health care services and how this compares with mainstream services. Another issue is achieving incomes for doctors in rural and remote locations that are competitive with incomes earned by GPs in metropolitan private practice.
The National Aboriginal and Torres Strait Islander Health Workforce Strategic Framework (2016–2023) provides a guide to assist planning, prioritising, target setting, monitoring and reporting of progress in Aboriginal and Torres Strait Islander health workforce capacity building. A key aim of the Framework is to improve recruitment and retention of Aboriginal and Torres Strait Islander health professionals in clinical and non-clinical roles across all health disciplines, including through ensuring workplace environments are culturally safe for Aboriginal and Torres Strait Islander health workers (see measure 3.12).
In 2015, the Australian Government released the Implementation Plan for the National Aboriginal and Torres Strait Islander Health Plan, which includes activities intended to deliver against the following strategy: Mainstream health services are supported to provide clinically competent, culturally safe, accessible, accountable and responsive services to Aboriginal and Torres Strait Islander peoples in a health system that is free of racism and inequality.
Aboriginal and Torres Strait Islander health professional organisations are funded to support and increase the capacity of the Indigenous workforce and contribute to promoting a culturally-appropriate health care system that contributes to improved access to services and improved outcomes for Indigenous Australians. They contribute to the recruitment and retention of Indigenous health professionals by providing mentoring, professional development, advice and practical support for their members and the broader Aboriginal and Torres Strait Islander health workforce.
The Remote Area Health Corps (RAHC) has been operating since 2008. It assists delivery of primary health care services in remote NT Indigenous communities by supplementing the efforts of the AMS and the NT Department of Health to recruit health professionals from urban-based practices and deploy them for short-term placements in remote NT communities, where health resources are in high demand. The RAHC is funded under the Indigenous Australians’ Health Programme (see Policies and Strategies section).
A programme to improve WA’s regional medical services was successful in supporting and retaining GPs with a 70% improvement in the GP retention rate at the four-year mark (OAG-WA, 2015).
Recognition of Aboriginal and Torres Strait Islander health as an identifiable specialty is also considered to be important in improving services and retaining highly skilled clinicians. Strong cooperation and collaboration between the health and education portfolios is vital for improving recruitment and retention of health staff.