3.06 Access to hospital procedures
Page content
Why is it important?
Studies have shown that while Indigenous Australians are more likely to be hospitalised than other people they are less likely to receive a medical or surgical procedure while in hospital (Cunningham, 2002; ABS & AIHW, 2008). The disparities are not explained by diagnosis, age, sex or place of residence (Cunningham, 2002). For patients admitted to hospital with coronary heart disease, access to coronary angiography can be important in diagnosis and establishment of a course of treatment. Coronary heart disease may be treated with medicines or through repairing the heart’s blood vessels, either using a medical procedure (percutaneous coronary interventions) or a surgical procedure (coronary artery bypass grafts). A study of patients admitted to Qld hospitals for acute myocardial infarction (heart attack) between 1998 and 2002 found that rates of coronary procedures among Indigenous Australian patients were 22% lower than rates for other patients (Coory & Walsh, 2005). A recent study in SA found that Indigenous patients were less likely to receive angiography after controlling for age, comorbidities and remoteness (Tavella et al, 2016).
Several studies have shown Aboriginal and Torres Strait Islander peoples have poorer survival rates for cancer. This is partly explained by later diagnosis and referral for specialist treatment (Condon et al, 2006; Valery et al, 2006). However, after controlling for stage of diagnosis Indigenous Australians are less likely to have treatment for cancer (surgery, chemotherapy, radiotherapy), tend to wait longer for surgery and have lower survival rates for many cancers (Valery et al, 2006; Hall, SE et al, 2004).
The proportion of Aboriginal and Torres Strait Islander people with end stage renal failure who received a kidney transplant was lower (11%) than other Australians (47%) (see measure 1.10).
Findings
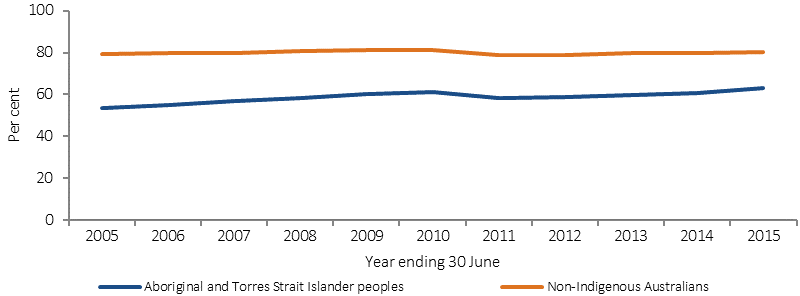
In the two years to June 2015, excluding care involving dialysis, 62% of hospital episodes for Aboriginal and Torres Strait Islander peoples had a procedure recorded, compared with 81% of hospital episodes for non-Indigenous Australians. There has been a significant increase in Indigenous hospitalisation rates with a procedure recorded between 2004–05 and 2014–15 in NSW, Vic, Qld, WA, SA and the NT combined. Over the same period there was a smaller significant increase in non-Indigenous rates, resulting in a significant decrease in the gap.
For Indigenous Australians, 7% of procedures were performed in private hospitals compared with 42% for non-Indigenous Australians in the two years to June 2015. There are many factors associated with the likelihood of receiving a procedure when admitted to hospital. An analysis of the combined impact of a range of factors found that between July 2013 and June 2015 the most significant factors (in order or importance) were:
- whether the hospital was a public or private hospital
- the number of additional diagnoses recorded for a patient
- the principal diagnosis for which a person was admitted
- state/territory of usual residence
- Indigenous status
- age group
- remoteness of usual residence
- sex.
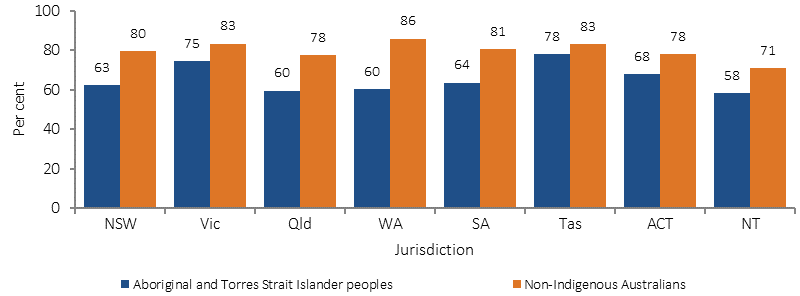
Across all age groups, Indigenous Australians were less likely to receive a procedure. Analysis by remoteness showed a decrease in hospitalisations with a procedure recorded as remoteness increased. The gap between the proportions of Indigenous and non-Indigenous Australians receiving a hospital procedure was highest in remote areas and lowest in major cities.
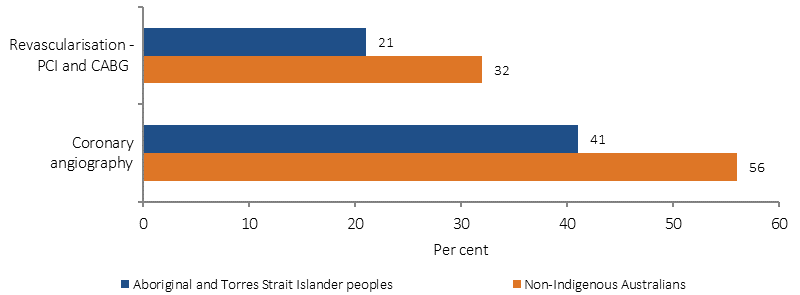
Between July 2013 and June 2015, among those hospitalised with coronary heart disease, Aboriginal and Torres Strait Islander people were around two-thirds as likely to receive coronary procedures such as coronary angiography and revascularisation procedures, compared with non-Indigenous Australians.
For hospitalisations related to diseases of the digestive tract between July 2013 and June 2015, the odds of Aboriginal and Torres Islander patients receiving a corresponding procedure were significantly lower than for non-Indigenous patients when the principal diagnosis was: complicated or uncomplicated hernias; diseases of the extrahepatic biliary tree; non-neoplastic diseases of the anus or rectum; and malignant neoplasms of the large intestine/rectum. There was no significant difference where the principal diagnosis was appendicitis.
Figures
Figure 3.06-1
Proportion of hospitalisations with a procedure reported (age-standardised), NSW, Vic, Qld, WA, SA and NT combined, 2004–05 to 2014–15
Source: AIHW analysis of National Hospital Morbidity Database
Table 3.06-1
Proportion of hospitalisations with a procedure reported, by principal diagnosis and Indigenous status, July 2013–June 2015
| Principal diagnosis chapter (excluding dialysis) | Indigenous | Non-Indigenous |
|---|---|---|
| Per cent | ||
| Diseases of the eye | 93 | 99 |
| Neoplasms | 91 | 96 |
| Diseases of the blood | 89 | 94 |
| Congenital malfunctions | 85 | 91 |
| Factors influencing health status | 78 | 94 |
| Diseases of the ear | 77 | 84 |
| Certain conditions in perinatal period | 74 | 74 |
| Diseases of the musculoskeletal system | 74 | 91 |
| Endocrine, nutritional & metabolic disorders | 69 | 84 |
| Diseases of the digestive system | 67 | 88 |
| Pregnancy and child birth | 66 | 79 |
| Diseases of the circulatory system | 65 | 74 |
| Diseases of the genitourinary system | 64 | 79 |
| Diseases of the skin | 63 | 71 |
| Diseases of the nervous system | 60 | 83 |
| Injury and poisoning | 60 | 70 |
| Infectious and parasitic diseases | 50 | 45 |
| Diseases of the respiratory system | 46 | 64 |
| Mental and behavioural disorders | 41 | 65 |
| Symptoms and signs and n.e.c. | 36 | 56 |
| Any principal diagnosis | 62 | 81 |
Source: AIHW analysis of National Hospital Morbidity Database
Figure 3.06-2
Proportion of hospitalisations with a procedure performed, by Indigenous status and state/territory (excluding care involving dialysis), July 2013–June 2015
Source: AIHW analysis of National Hospital Morbidity Database
Figure 3.06-3
Age-standardised use of coronary procedures for those hospitalised with coronary heart disease, by Indigenous status, July 2013–June 2015
Source: AIHW analysis of National Hospital Morbidity Database
Implications
Disparities in hospital procedures are likely to reflect a range of factors, including ‘systemic practices, not ill-intentioned but still discriminatory, and almost invisible in the patient provider encounter’ (Fisher & Weeramanthri, 2002). An adequate primary health care system is also a prerequisite for effective hospital and specialist services.
In the 2014–15 Social Survey, 36% of Indigenous adults had incomes in the bottom 20% of Australian incomes. In the 2012–13 Health Survey, 20% of Indigenous Australians in non-remote areas reported they had private health insurance with the main barrier being affordability (72%). The lower proportion of procedures per hospitalisation is likely to be associated with private health insurance coverage and lower access to private hospitals. This may have impacts on the rate of preventative hospital treatments. A recent study found that, after adjusting for other factors, the strongest association with coronary angiography rates was admissions to private hospitals (Chew et al, 2016).
Aboriginal and Torres Strait Islander patients with chronic disease sometimes present later in the course of these illnesses, compared with non-Indigenous Australians, which affects treatment options (Valery et al, 2006). Other factors that have been suggested include: that the presence of comorbidities limits treatment options (although this does not explain the difference in coronary procedures outlined above); clinical judgments concerning post-procedural compliance; communication issues, such as for patients whose main language is not English; and patient knowledge and attitudes, e.g. fatalistic attitudes towards cancer. Physical, social and cultural distance from health services also play a role, along with financial issues patients and their families may face when seeking treatment in specialist referral services (Shahid et al, 2009; Miller et al, 2010). Analysis of 2015–16 Medicare data shows that the rate of claims for specialist services for Aboriginal and Torres Strait Islander peoples was below national averages for both in and out of hospital care. Effective strategies will require a better understanding of the factors leading to the observed disparities.
The measures presented here suggest that under-provision of specialist services for Indigenous Australians persists, and that further efforts are required to improve access. In addition to governments, clinicians and clinical colleges could also play a role in reviewing decision-making processes and relevant data to identify what drives differential access to procedures and develop strategies to address these issues (Fisher & Weeramanthri, 2002).
Heart and cardiovascular conditions make the greatest contribution to the life expectancy gap. The National Recommendations for Better Cardiac Care for Aboriginal and Torres Strait Islander People and the Lighthouse Hospital Project (see measure 1.05) aim to address the disparities in cardiovascular care. Under the former Health and Hospitals Fund, funding was provided to the NT Government for three projects to improve access to hospital procedures, including: $13.6 million for an Emergency Department at the Alice Springs Hospital; $3.7 million to upgrade the Emergency Department at Tennant Creek; and $18.6 million for accommodation (50 beds) at Royal Darwin Hospital for patients and carers from remote communities.
Survival rates of Aboriginal people with end stage kidney disease that require renal replacement therapy has significantly increased and recent evidence suggests the gap has closed between Aboriginal and non-Aboriginal patients. However, whilst this may be the case, differences still exist when adjusting for age.
The ACT Aboriginal and Torres Strait Islander Health Plan 2016–2020 aims to improve access to health and health care services.