1.20 Infant and child mortality
Page content
Why is it important?
Infant mortality is the death of a child less than one year of age and is a long established measure of child health, as well as the overall health of the population and its physical and social environment. COAG has committed to halving the gap in mortality rates for Aboriginal and Torres Strait Islander children under 5 years by 2018. Improvements in Australia’s infant mortality rates in the last 100 years were largely due to improved social and public health conditions such as sanitation and health education in the first half of the twentieth century, followed by the development of immunisation, and in more recent years by better treatment in neonatal intensive care and interventions for Sudden Infant Death Syndrome (SIDS).
Findings
Infant deaths contribute substantially to total years of life lost (YLL) due to premature mortality for Indigenous Australians, accounting for 11% of the total YLL in 2011 (AIHW, 2016f).
Between 1998 and 2015 there has been a significant decline in Indigenous child mortality rates of 33% and a significant narrowing of the gap (by 31%) with non-Indigenous children in jurisdictions with reliable data (NSW, Qld, WA, SA and the NT). In the 5-year period 2011–15, there were 610 deaths of Aboriginal and Torres Strait Islander children aged 0–4 years, and of these, 500 were infant deaths (82%). The mortality rate for Aboriginal and Torres Strait Islander children aged 0–4 years was 2 times the non-Indigenous rate (164.9 per 100,000 compared with 80.1 per 100,000).
In the period 2011–15, the mortality rate for Indigenous infants was 1.9 times the non-Indigenous rate (6.1 per 1,000 live births compared with 3.3 per 1,000 live births). The Indigenous infant mortality rate has more than halved, from 13.5 to 6.3 per 1,000 live births, between 1998 and 2015. The gap between mortality rates for Indigenous infants and non-Indigenous infants narrowed significantly (by 84%). In 2011–15, Aboriginal and Torres Strait Islander infant mortality rates varied across jurisdictions, from 4 per 1,000 in NSW, to 14 per 1,000 in the NT. A study in Victoria involving data linkage to improve the quality of Indigenous identification found the Indigenous infant mortality rate was nearly twice the rate for non-Indigenous infants (Freemantle et al, 2014). Data on trends from 1967 to 2006 in the NT (the only jurisdiction with adequate data quality for this period) show an 81% fall in the Indigenous infant mortality rate with rapid declines until the mid-1980s, followed by slower improvement over the past 20 years. There has been substantial improvement in the NT during the period 1967 to 2006 for both neonatal death rates (up to age 28 days) and post-neonatal death rates (from 28 days to one year) (Wang & Li, 2010).
In 2011–15 the most common causes of death for Aboriginal and Torres Strait Islander infants were conditions originating in the perinatal period (51%) such as birth trauma, fetal growth disorders, complications of pregnancy, and respiratory and cardiovascular disorders specific to the perinatal period. The second leading cause of death was signs, symptoms and ill-defined conditions (21%). This category includes SIDS, which accounted for 8% of infant deaths. The third most common cause of Indigenous infant deaths was congenital malformations accounting for 13% of infant deaths. Among older Indigenous children aged 1–4 years, injury accounted for half of the deaths, and the rate for Indigenous children was 4 times as high as the non-Indigenous rate. Nearly half of the decline in Indigenous infant mortality over the last decade is due to a reduction in deaths from signs, symptoms and ill-defined conditions (including SIDS) and certain conditions originating in the perinatal period (such as complications of pregnancy, labour and delivery, fetal growth disorders, infections and respiratory and cardiovascular disorders).
A retrospective study of infants with congenital heart defects born in WA (1980–2010) found that long-term survival was lower for Indigenous than non-Indigenous children, with increased mortality risk likely due to socio-economic and environmental factors (Nembhard et al, 2016).
International statistics show that indigenous infants in the US and New Zealand have higher mortality rates than infants in the general population and these gaps are similar to the gap between Aboriginal and Torres Strait Islander and non-Indigenous infants. In New Zealand the infant mortality rate for Maoris was 6 per 1,000 live births compared with 4 per 1,000 for other infants in 2012. In the United States, the mortality rate for American Indians/Alaskan Natives was 8 per 1,000 live births compared with 6 per 1,000 live births for the total population in 2013. Caution must be used in comparing data with other countries due to variations in data quality, methods applied for addressing data quality issues and definitions for identifying indigenous peoples.
Figures
Figure 1.20-1
Infant mortality rates per 1,000 live births, by Indigenous status, NSW, Qld, WA, SA and the NT, 1998 to 2015
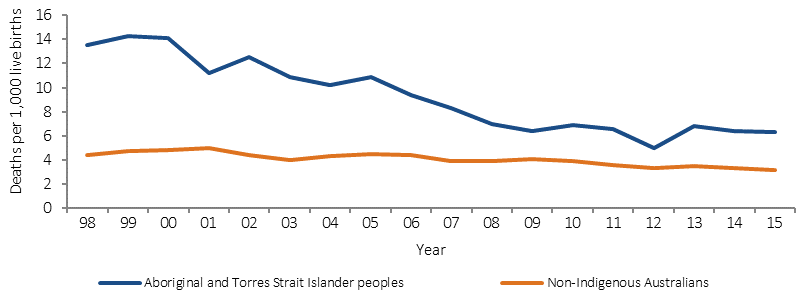
Source: ABS and AIHW analysis of National Mortality Database
Figure 1.20-2
Infant mortality rates per 1,000 live births, by Indigenous status, NT, 1967 to 2006(a)
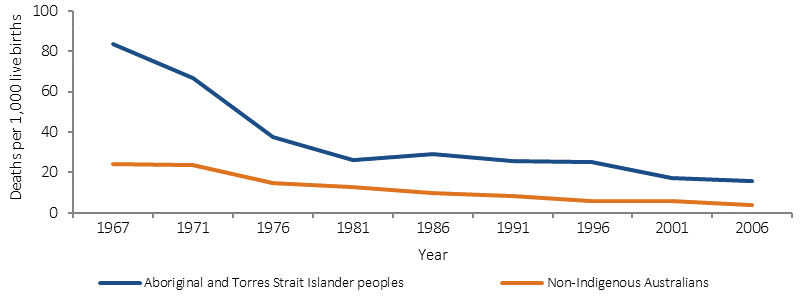
(a) Rates are for 4 and 5-year averages
Source: Wang, 2010
Table 1.20-1
Infant mortality rates per 1,000 live births, by Indigenous status, NSW, Qld, WA, SA and the NT, 2011–15
| Jurisdiction | Number of deaths | Rate per 1,000 live births | Ratio | Rate Difference | ||
|---|---|---|---|---|---|---|
| Indigenous | Non-Indigenous | Indigenous | Non-Indigenous | |||
| NSW | 118 | 1,581 | 4.0 | 3.3 | 1.2 | 0.6 |
| Qld | 175 | 1,183 | 6.7 | 4.1 | 1.6 | 2.6 |
| WA | 77 | 327 | 5.6 | 2.1 | 2.7 | 3.5 |
| SA | 31 | 257 | 6.5 | 2.7 | 2.4 | 3.8 |
| NT | 99 | 45 | 13.8 | 3.4 | 4.0 | 10.4 |
| Total of 5 jurisdictions | 500 | 3,393 | 6.1 | 3.3 | 1.9 | 2.8 |
Source: ABS and AIHW analysis of National Mortality Database
Table 1.20-2
Infant mortality rates per 1,000 live births, by Indigenous status, NSW, Qld, WA, SA and the NT, 2011–15
| Cause of death | Number of deaths | Rate per 1,000 live births | Ratio | Rate difference | ||
|---|---|---|---|---|---|---|
| Indigenous | Non-Indigenous | Indigenous | Non-Indigenous | |||
| Certain conditions originating in the perinatal period | 256 | 1,774 | 3.1 | 1.7 | 1.8 | 1.4 |
| Signs, symptoms & ill-defined conditions | 103 | 357 | 1.3 | 0.3 | 3.6 | 0.9 |
| SIDS (subcategory of Signs, symptoms etc) | 39 | 157 | 0.5 | 0.2 | 3.1 | 0.3 |
| SUDI (subcategory of Signs, symptoms etc) | 64 | 199 | 0.8 | 0.2 | 4.1 | 0.6 |
| Congenital malformations | 67 | 816 | 0.8 | 0.8 | 1.0 | — |
| Other conditions | 19 | 212 | 0.2 | 0.2 | 1.1 | — |
| Diseases of the respiratory system | 20 | 48 | 0.2 | — | 5.2 | 0.2 |
| Infectious and parasitic diseases | 11 | 51 | 0.1 | — | 2.7 | 0.1 |
| Injury and poisoning | 19 | 84 | 0.2 | 0.1 | 2.8 | 0.2 |
| Diseases of the circulatory system | 5 | 51 | 0.1 | — | 1.2 | — |
| Total | 500 | 3,393 | 6.1 | 3.3 | 1.9 | 2.8 |
Source: ABS and AIHW analysis of National Mortality Database
Implications
Both child and infant Indigenous mortality rates are declining. While mortality for non-Indigenous children is also declining, the gaps in mortality between Indigenous and non-Indigenous infants and children are reducing. Deaths during the neonatal period (up to 28 days), which account for 62% of infant deaths, have also fallen significantly (see measure 1.21). This significant improvement provides opportunities to understand which aspects of Aboriginal and Torres Strait Islander lives contribute to infant and child mortality, and where the health system could be more effective in engaging with Aboriginal and Torres Strait Islander peoples to support healthy pregnancies and childhood development.
The key risk factors associated with infant and child mortality include low birthweight and pre-term births, maternal health and behaviours (nutrition during pregnancy, smoking, alcohol), socio-economic status, and access to health services (AIHW, 2014b). Studies have shown an association between inadequate antenatal care and an increase of these risk factors, so improved access to, and take up of, antenatal care services is crucial for improving child outcomes (Taylor, LK et al, 2013). There have been improvements for Indigenous Australians for several of these risk factors in recent years, for example a 13% decline in low birthweight from 2000 to 2014 (see measure 1.01). However, there remains a significant disparity between the Indigenous and non-Indigenous rates of antenatal care in the first trimester (8 percentage points less), smoking during pregnancy (4 times higher), low birthweight (2 times higher for Indigenous) and immunisation at age 1 (4 percentage points lower).
A study of avoidable mortality in the NT between 1985 and 2004 found the largest improvements in deaths were for conditions amenable to medical care such as increased number of births in hospital, improved neonatal and paediatric care and the establishment of pre-natal screening for congenital abnormalities (Li, SQ et al, 2009). The long-term study in the NT from 1967 found improvements in both neonatal deaths (usually indicative of pregnancy related health and services) and post-neonatal deaths (indicative of conditions) (Wang & Li, 2010).
In December 2007, COAG committed to closing the gap in Indigenous disadvantage and, in particular, to halving the gap in mortality rates for Aboriginal and Torres Strait Islander children under 5 years of age by 2018. Australian governments are investing in a range of initiatives to improve child and maternal health.
The 2014–15 Federal Budget provided funding of $94 million from July 2015 for the Better Start to Life approach to expand efforts in child and maternal health to support Indigenous children to be healthy and ready for school.
The Better Start to Life approach included $54 million to increase the number of New Directions: Mothers and Babies services from 85 to 136. These services provide Aboriginal and Torres Strait Islander families with access to antenatal care, practical advice and assistance with parenting, and health checks for children.
This approach also provides $40 million to expand the Australian Nurse–Family Partnership Program (ANFPP) from 3 to 13 sites. The ANFPP aims to improve pregnancy outcomes by helping women engage in good preventive health practices, support parents to improve their child's health and development, and help parents develop a vision for their own future, including continuing education and finding work.
The Indigenous Australians’ Health Program has allocated $12 million over two years (from July 2016) to support the implementation of integrated early childhood services: Connected Beginnings, as recommended by the Forrest Review. The Department of Education has also allocated $30 million over three years to support the programme, which will support integrated health and education services for antenatal to school age children.
The Foetal alcohol spectrum disorder (FASD) prevention program is a project in the Kimberly region run by the Ord Valley Aboriginal Health Service. The programme applies innovative strategies in providing education and support of antenatal clients and their families, as well as providing regular education sessions to students in the region.
In SA, the Aboriginal Family Birthing Program (a partnership model between Aboriginal Maternal Infant Care Workers and midwives) supports Aboriginal women and their families through pregnancy, childbirth and up to 6 weeks postnatally. Since its inception in 2004, SA has seen, for women in the Program, a significant decrease in low birthweight rates, infant mortality and in the proportion of Aboriginal mothers smoking during pregnancy.