2.18 Physical activity
Page content
Why is it important?
Physical activity can be defined as a bodily movement produced by the muscles resulting in energy expenditure, and can include organised or incidental activity (AIHW, 2010a). Physical inactivity is an important modifiable risk factor associated with several potentially preventable chronic diseases that are prevalent in the Aboriginal and Torres Strait Islander population. These diseases include cardiovascular disease, cancer, stroke, hypertension and diabetes (Gray, C et al, 2013; Wilmot et al, 2012; AIHW, 2012b).
Physical inactivity is also related to overweight and obesity, another important risk factor for multiple preventable diseases.
In 2011, physical inactivity accounted for 5.5% of the total burden of disease in the Indigenous population and 8.2% of the health gap with non-Indigenous Australians (AIHW, 2016f). Physical inactivity is the fourth leading risk factor in the Indigenous population, after smoking, alcohol and high body mass. Its effect is manifested through a range of diseases. Notably, this study found that 44% of the coronary heart disease burden and also 36% of the diabetes burden were attributable to physical inactivity.
Current guidelines (Dept. of Health, 2017) recommend that children aged 2–4 years are physically active for at least 3 hours every day; that children aged 5–17 years do at least 60 minutes per day of moderate to vigorous intensity physical activity; that adults aged 18–64 years accumulate 150 to 300 minutes (2 ½ to 5 hours) of moderate intensity physical activity or 75 to 150 minutes (1 ¼ to 2 ½ hours) of vigorous intensity physical activity per week; and that adults aged over 65 years accumulate at least 30 minutes of moderate intensity physical activity on most days. The guidelines also recommend minimal time spent sitting (sedentary behaviour) for all ages. Katzmarzyk et al. (2009) found an increased risk of mortality with higher levels of sitting time regardless of whether sufficient physical activity was undertaken.
Research has established inverse associations between physical activity with fat mass and biomedical risk factors for chronic disease (Ness et al, 2007; Steele et al, 2009; White, SL et al, 2011), and studies have confirmed that activity reduces the risk for heart disease (Stephenson et al, 2000; Bull et al, 2004; Sattelmair et al, 2011), high blood pressure (Kokkinos et al, 2001), diabetes (NHF, 2006) and the symptoms of depression, anxiety and stress (WHO, 2010; Moylan et al, 2013)(WHO 2010; Moylan et al. 2013). Physical activity has physical and psychological benefits for the management and treatment of chronic conditions (Adami et al, 2010; Holmes et al, 2005; NHF, 2006).
Findings
The most recent data on physical activity is from the 2012–13 Health Survey, which collected information on walking for exercise/transport and moderate and vigorous physical activity in the week prior. While information was collected in both remote and non-remote areas, results are not comparable due to differing methodologies across areas.
In 2012–13, 38% of Indigenous adults in non-remote areas had undertaken a sufficient level of physical activity in the week prior (at least 150 minutes over 5 or more sessions). Rates of sufficient activity were higher for Indigenous males (43%) than for Indigenous females (33%). After adjusting for differences in the age structure of the two populations, Indigenous adults were less likely than non-Indigenous adults to have met sufficient activity levels in the last week (rate ratio of 0.8), and more likely to be inactive (rate ratio of 1.3). Younger Indigenous Australians were more likely to be sufficiently active and activity levels declined with age; 48% aged 18–24 years were sufficiently active compared with 27% aged 55 years and over.
After adjusting for differences in the age structure between the two populations, Indigenous adults spent 1.7 times the time walking for transport than non-Indigenous adults (average of 143 minutes compared with 83 minutes per week) and less time on walking for fitness (0.8 times) and moderate or vigorous physical activity (0.7 and 0.8 times respectively). Indigenous adults spent 1.3 times the time spent by non-Indigenous adults on watching television or videos and less time using a computer/internet (0.6 times) and sitting for transport (0.8 times). In a pedometer study done as part of 2012–13 Health Survey, 17% of Indigenous adults did the required 10,000 steps per day on average. More than half (55%) of Indigenous adults in remote areas spent more than 30 minutes in the previous day undertaking physical activity/walking; 20% spent less than 30 minutes and 21% did no physical activity.
In 2012–13, 82% of Aboriginal and Torres Strait Islander children aged 2–4 years in non-remote areas met the recommendations of at least 3 hours of physical activity per day. Average time spent in physical activity was similar for Indigenous and non-Indigenous children aged 2–4 years, although Indigenous children spent more time outdoors (3.5 hours compared with 2.8 hours per day on average).
Nearly half (48%) of Indigenous children aged 5–17 years in non-remote areas met the recommended physical activity guidelines, at a much higher rate than for non-Indigenous children (35%). Indigenous children were 1.4 times as likely as non-Indigenous children to have met both the physical activity and screen-based guidelines in the three days prior (25% compared with 18%). One in four Indigenous children met the threshold of 12,000 steps per day (on average), similar to non-Indigenous children. In 2012–13, 82% of Aboriginal and Torres Strait Islander children aged 5–17 years in remote areas did more than 60 minutes of physical activity on the day prior (only 4.1% did no physical activity).
Aboriginal and Torres Strait Islander adults who were sufficiently active were less likely to be obese (31%) than those who were inactive (56%). Indigenous adults with educational qualifications of Year 12 or above were 1.5 times as likely to have done sufficient physical activity as those with below Year 10 (44% compared with 29%). Indigenous adults in non-remote areas who described their health as excellent or very good were 1.7 times as likely to have done sufficient physical activity as those with fair/poor self-assessed health.
Figures
Figure 2.18-1
Persons aged 18 years and over, level of physical activity, by Indigenous status, non-remote areas, 2012–13
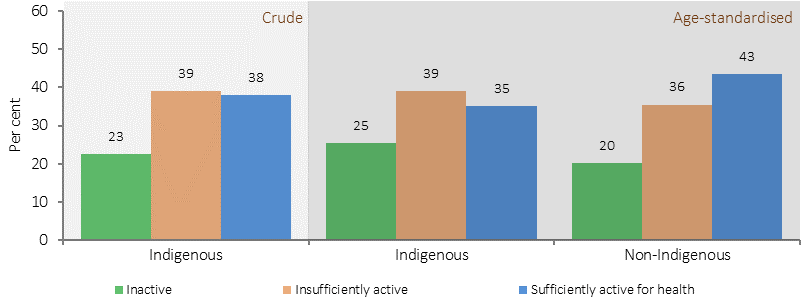
Source: 2012–13 AATSIHS (ABS, 2014)
Figure 2.18-2
Indigenous persons aged 18 years and over reporting a sufficient level of physical activity, by age-group and sex, non-remote areas, 2012–13
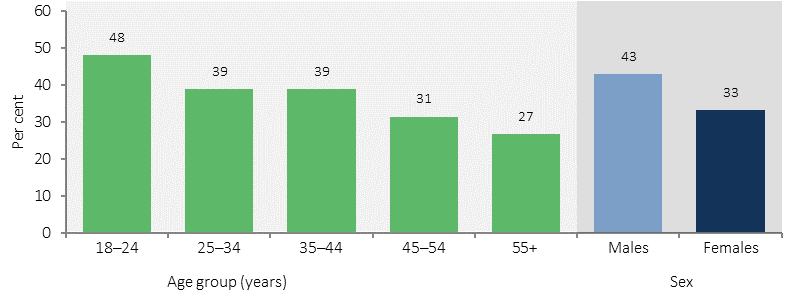
Source: 2012–13 AATSIHS (ABS, 2014)
Figure 2.18-3
Persons aged 5–17 years, whether met physical activity recommendations by Indigenous status, non-remote areas, 2012–13
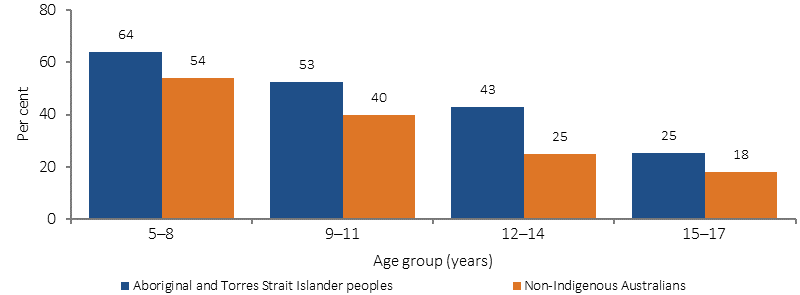
Source: 2012–13 AATSIHS (ABS, 2014)
Figure 2.18-4
Persons aged 5–17 years, whether met screen-based activity recommendations by Indigenous status, non-remote areas, 2012–13
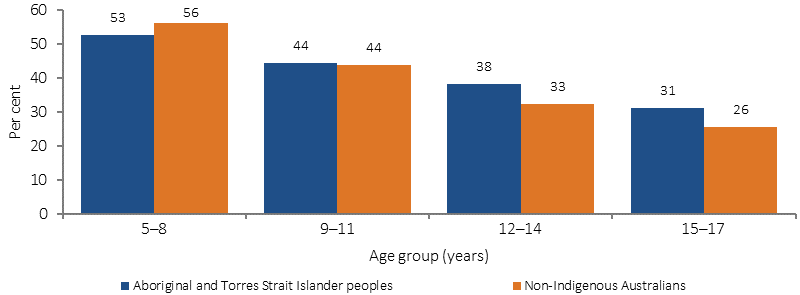
Source: 2012–13 AATSIHS (ABS, 2014)
Implications
Low levels of physical activity were reported by nearly 3 in 5 Aboriginal and Torres Strait Islander people aged 18 years and over in non-remote areas in 2012–13. Higher rates of sedentary behaviours are associated with an increased risk of chronic disease. Improving levels of physical activity presents a significant opportunity for health improvements and for reducing the health gap between Indigenous and non-Indigenous Australians.
Thompson et al. (2013) found that the concept of physical activity in remote NT communities was strongly linked to land and resource management and seasonal, family and cultural activities. Several studies have shown that high levels of incidental exercise can have health benefits (Ekblom-Bak et al, 2014; Samitz et al, 2011; Duvivier et al, 2013).
Under the Safety and Wellbeing Programme (part of the Indigenous Advancement Strategy), funding is provided to support community participation in sport and active recreation activities to bolster improved health and physical wellbeing outcomes, along with broader social benefits for participants and their communities. The programme's objectives are: reduced substance misuse and harm; crime prevention, diversion and rehabilitation; violence reduction and victim support; safe and functional environments and social and emotional wellbeing.
Participation in community sports and recreation programmes can have many positive benefits, including: improvements in school retention; attitudes towards learning, social and cognitive skills; physical and mental health and wellbeing; increased social inclusion and cohesion; increased validation of and connection to culture; and crime reduction (Ware & Meredith, 2013).
The National Aboriginal and Torres Strait Islander Health Plan (2013–2023) Implementation Plan includes identifying new evidence-based research and strategies to support physical activity choices.
The Australian Government revised physical activity and sedentary behaviour guidelines for children, young people and adults in February 2014 following a review of the recent and best available evidence concerning the relationship between physical activity, sedentary behaviour and a range of health outcome indicators, including the risk and prevention of chronic disease and obesity.
Move Well Eat Well (primary schools and early childhood settings) in Tasmania aims to improve the policies and practices in these settings to support nutrition and physical activity.
Increased physical activity opportunities are available in disadvantaged communities through implementation of the Get Active Program. A systematic review and meta-analysis demonstrated that programmes with a group delivery mode significantly increase physical activity among women experiencing disadvantage and group delivery should be considered an essential element of physical activity promotion programmes targeting this population group.