3.17 Regular GP or health service
Page content
Why is it important?
Having a usual primary health care provider is associated with good communication between the patient and provider, greater levels of trust and satisfaction with providers (Mainous et al, 2001; Schers et al, 2005), and better health outcomes for patients (Starfield, 1998; Starfield & Shi, 2004). Those with a usual primary care provider are more likely to receive: care based on guidelines, preventative care, and better coordination of care with other providers to meet patient need (Forrest & Starfield, 1996; Atlas et al, 2009). Other benefits of having a continuous doctor–patient relationship include improved diagnoses, better medication management, avoidance of repeat tests or other interventions, and fewer hospitalisations, particularly for people with complex health care needs (Hollander et al, 2009).
Findings
Based on self-reported 2012–13 Health Survey data, 86% of Aboriginal and Torres Strait Islander peoples have a usual place to go for health problems and advice. Most Indigenous Australians usually went to a doctor if they had a problem with their health (54%), followed by Aboriginal Medical Services (AMS) (17%), community clinics (10%) and hospitals (5%). Note: some caution is needed as respondents may not clearly differentiate between an AMS and a community clinic (ABS, 2013c) or between a doctor at an AMS or another practice (it is estimated that 3% of those that usually went to a ‘doctor’ went to an AMS doctor).
In 2012–13, 14% of Indigenous Australians had no regular source of health care. Use of AMSs and community clinics increased by remoteness, from 13% in major cities to 66% in very remote areas.
The survey asked where people would like to go if they were sick or needed advice about their health. In 2012–13, 53% of Indigenous Australians reported they would prefer to go to a doctor, 26% to an AMS, and 9% to a community clinic. In most instances Indigenous Australians expressed a preference for the services they currently use and services available in their local area. Preferences varied by remoteness with GPs preferred mostly by Indigenous Australians in major cities (68% compared with 10% in very remote areas) and community clinics preferred mostly by Indigenous Australians in very remote areas (50% compared with 2% in major cities).
Nationally, 27% of Indigenous Australians who said they would like to go to an AMS did not have an AMS available in their local area.
Availability of services varied across Australia. Around 95% of those living in major cities reported GPs being available compared with 31% in very remote areas. AMSs were reported as being locally available by 61% of those living in outer regional areas and 26% of those in very remote areas. In 2012–13, 77% of Indigenous Australians living in very remote areas reported that there were community clinics available compared with 33% of those living in major cities.
Nationally, 5% of Aboriginal and Torres Strait Islander peoples usually go to hospital if there is a problem with their health. See measure 3.07 for analysis of hospitalisations for conditions that could be prevented if primary health care services were better able to meet the needs of Aboriginal and Torres Strait Islander peoples. A higher use of hospitals for regular health care was reported in WA and Qld (both 10%) than in other jurisdictions (1%–3%).
In 2012–13, 70% of Aboriginal and Torres Strait Islander peoples rated their health care experience as ‘excellent’ or ‘very good’ in the previous 12 months. Indigenous Australians with no usual GP/medical service reported lower rates of satisfaction than those with a regular doctor/GP (61% reporting excellent or very good compared with 73%).
In 2012–13, the majority of Indigenous Australians aged 15 years and over living in non-remote areas reported that doctors listened to them (89%), explained things in a way that could be understood (87%), showed respect for what was said (89%) and spent enough time with them (85%). National data for all Australians from the Patient Experience Survey showed that GPs always or often listened carefully (89%), showed respect (93%) and spent enough time with them (88%) (SCRGSP, 2013).
In the 2014–15 Social Survey, 35% of Indigenous Australians reported they had been treated unfairly in the previous 12 months because they are Aboriginal or Torres Strait Islander. Around 2% of Indigenous people avoided seeking care from doctors, nurses or other staff at hospitals or doctor’s surgeries because of previous unfair treatment.
In 2014–15, around 81% of Indigenous Australians aged 15 years and over agreed/strongly agreed that their doctor can be trusted. Further analysis of this issue is discussed in the context of cultural competency (see measure 3.08).
Figures
Figure 3.17-1
Usual source of health care by type, Indigenous Australians, by remoteness, 2012–13
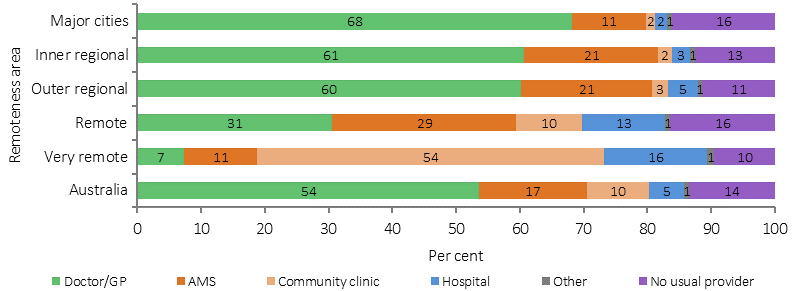
Source: ABS and AIHW analysis of 2012–13 AATSIHS
Figure 3.17-2
Preferred source of health care by type, Indigenous Australians, by remoteness, 2012–13
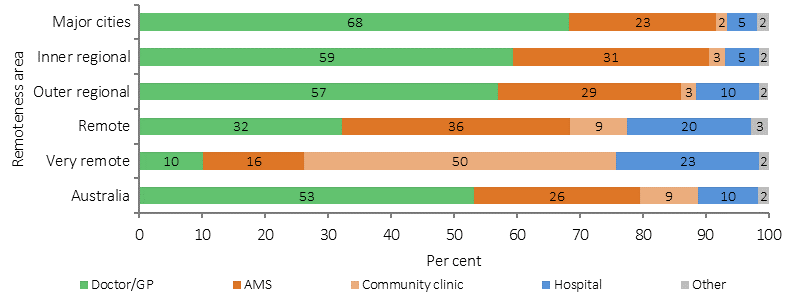
Source: ABS and AIHW analysis of 2012–13 AATSIHS
Figure 3.17-3
Available sources of health care by type, Indigenous Australians, by remoteness, 2012–13
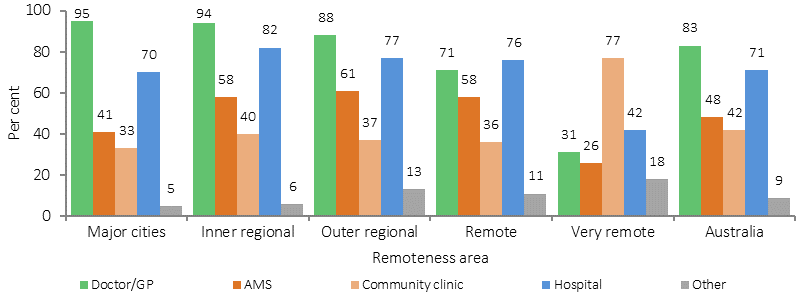
Source: ABS and AIHW analysis of 2012–13 AATSIHS
Figure 3.17-4
Patient experience by usual source of health care, Indigenous Australians 15 years and over who saw a doctor or specialist (non-remote) 2012–13
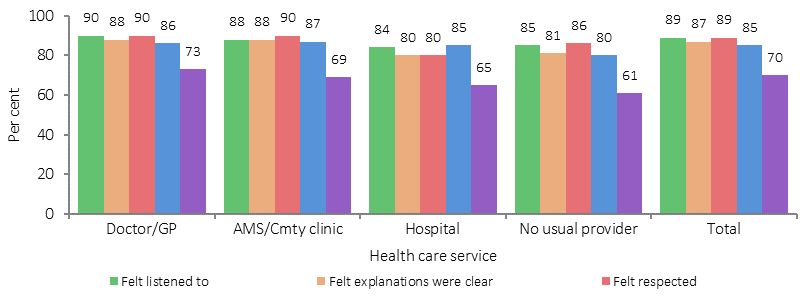
Source: ABS and AIHW analysis of 2012–13 AATSIHS
Implications
Most Aboriginal and Torres Strait Islander peoples have a usual source of health care. This finding is encouraging as access to a usual source of care is one of the foundations for a good primary health care system. The main sources of primary health care for Indigenous Australians are GPs, AMSs and community clinics. While mainstream general practice is a significant source of care for Indigenous Australians, for most GPs, Indigenous clients will remain a small proportion of their clients. Some mainstream practices have implemented strategies explicitly focused on their Indigenous patients (Hayman, NE et al, 2009; Spurling et al, 2009).
Australian Government initiatives include the Practice Incentives Program—Indigenous Health Incentive (PIP–IHI) to support general practices and Indigenous health services to provide better health care for Aboriginal and Torres Strait Islander patients. Payments are made to practices that register for the PIP–IHI and meet certain requirements, including establishing and using a mechanism to ensure Indigenous patients aged 15 years and over with a chronic disease are followed up (e.g. use of a recall/reminder system or staff actively seeking out patients to ensure they return for ongoing care), and at least two staff members from the practice (one of whom must be a GP) completing appropriate cultural awareness training. In 2014–15, about 3,700 general practices and Indigenous health services had signed on to the incentive. Around 64,700 patients were registered in 2014–15 (Department of Health unpublished).
The Australian Government is continuing to ensure high quality training is provided to GP registrars under the Australian General Practice Training Program, and supports 1,500 commencing GP registrars each year as well as ongoing participants. At least 50% of all GP training is undertaken in rural and regional areas.