3.18 Care planning for chronic diseases
Page content
Why is it important?
Chronic diseases are the major causes of illness, disability and death among Aboriginal and Torres Strait Islander peoples (see measures 1.02 and 1.23) and are estimated to be responsible for 70% of the health gap (AIHW, 2016f).
Effective management of chronic disease can delay the progression of disease, decrease the need for high-cost interventions, improve quality of life, and increase life expectancy. As good quality care for people with chronic disease generally involves multiple health care providers across multiple settings, the development of care plans is one way in which the client and primary health care (PHC) provider can ensure appropriate care is arranged and coordinated.
A care plan is a written action plan containing strategies for delivering care that address an individual’s specific needs, particularly patients with chronic conditions and/or complex care needs. A care plan can be used to record information about the patient’s condition, actions the patient needs to take and the various services required to achieve management goals for the patient. Development of a care plan can also help encourage the patient to take informed responsibility for their care, including actions to help achieve the treatment goals. A care plan may involve one health professional (usually a GP or other PHC doctor), or may be negotiated with several service providers (e.g. GP, nurse, Aboriginal health worker, allied health professionals, community services providers) in consultation with the patient.
A number of reviews have found that the chronic disease interventions most likely to be effective in the Australian context include: engaging primary care services in self-management support through education and training for GPs and practice nurses, and including self-management support in care plans linked to multidisciplinary team support (Kowanko et al, 2012; Dennis et al, 2008).
GPs are encouraged to develop care plans through a number of items under the Medicare Benefits Schedule. In July 2005, Chronic Disease Management items were introduced specifically focused on patients with chronic or terminal conditions who will benefit from a structured approach to management of their care needs. These include an item related to the development of a GP Management Plan (GPM), an item for a Team Care Arrangements (TCA) where planning involves a broader team, and items for where GPs contribute to care plans developed by another service provider or to a review of those plans.
Findings
In 2015–16, there were nearly 66,100 Medicare GPMP claims and 56,400 TCA claims for Indigenous Australians—a steady increase in uptake since these items were introduced in July 2005. In the period 2009–10 to 2015–16, rates of services claimed by Indigenous Australians have doubled for TCAs (from 55 to 112 per 1,000) and almost doubled for GPMPs (from 70 to 129 per 1,000).
In 2015–16, the Indigenous rate was higher than the non-Indigenous rate for both GPMPs (129 per 1,000 compared with 86 per 1,000) and TCAs (112 per 1,000 compared with 72 per 1,000). This higher rate for Indigenous Australians has been particularly noticeable from 2009–10 when the Indigenous chronic disease initiatives were introduced.
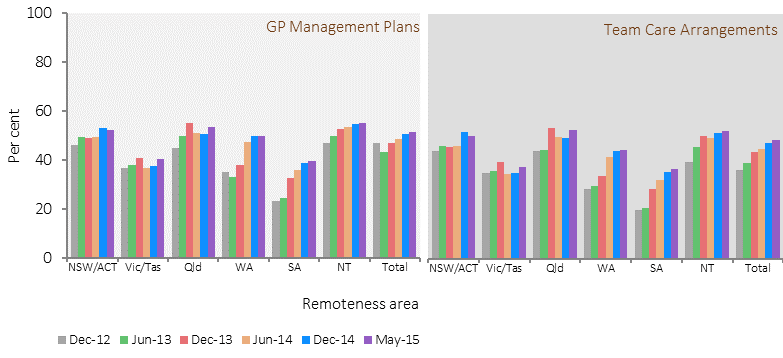
Commonwealth-funded Indigenous PHC organisations provide national Key Performance Indicators (nKPI) data on a range of process of care measures related to chronic disease management. In May 2015, around 32,900 regular Indigenous clients of these organisations had Type 2 diabetes. Of these clients, 51% had a GPMP in the two years to May 2015. This was an increase of 10 percentage points from December 2012. Improvements were seen in all jurisdictions and remoteness areas.Of clients with diabetes, 48% had a TCA in the two years to May 2015. This was an increase of 12 percentage points from December 2012. Improvements were again seen nation-wide.
In 2014–15, Commonwealth-funded Indigenous PHC organisations provided organisation-level data on chronic disease management. All 203 organisations provided some form of care planning. In particular, 67% reported that discharge planning was well coordinated and 70% provided or facilitated shared-care arrangements for managing people with chronic conditions.
Key elements of effective asthma management include a written asthma action plan and regular use of medications that control the disease and prevent exacerbations of the condition (AIHW, 2011b). Based on self-reported data from the 2012–13 Health Survey, 29% of Indigenous Australians with asthma living in non-remote areas had a written asthma action plan (similar to the proportion for non-Indigenous Australians, after adjusting for differences in the age structures of the two populations). Rates were highest for children aged 0–14 years. Indigenous Australians were more likely to go to hospital or an emergency department due to their asthma than non-Indigenous Australians, particularly in the age groups over 25 years. In 2012–13, an estimated 18% of Indigenous Australians had asthma—twice the non-Indigenous rate.
Figures
Figure 3.18-1
Age-standardised rates of selected GPMPs and TCAs claimed through Medicare by Indigenous status, 2005–06 to 2015–16
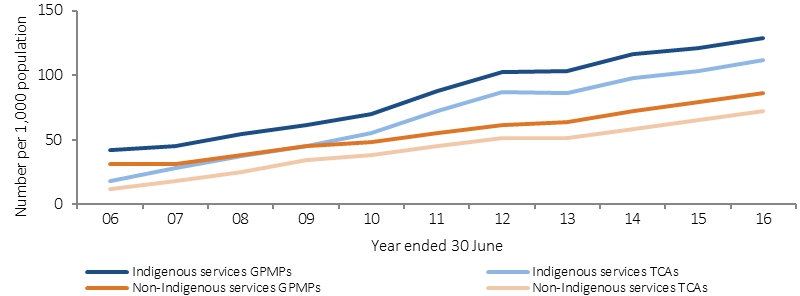
Source: Medical Benefits Division, Department of Health
Figure 3.18-2
Proportion of people with asthma reporting having a written asthma action plan, by Indigenous status and age group, non‑remote areas, 2012–13
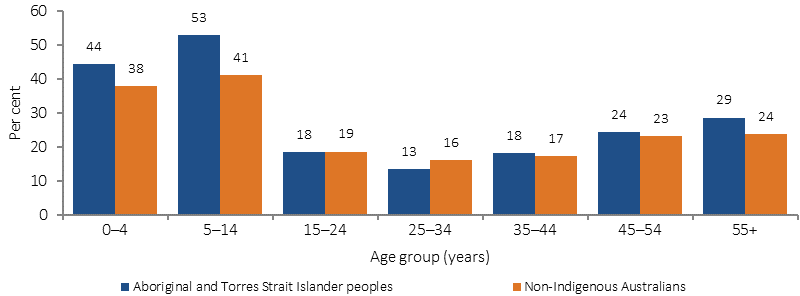
Source: ABS and AIHW analysis of 2012–13 AATSIHS
Figure 3.18-3
Proportion of Indigenous regular clients with type 2 diabetes who had a GPMP and TCA in the last 2 years, by remoteness area, Indigenous primary health care organisations, December 2012, June 2013, December 2013, June 2014, December 2014 and May 2015

Source: AIHW analysis of national Key Performance Indicators for Aboriginal and Torres Strait Islander primary health care data collection
Figure 3.18.4
Proportion of Indigenous regular clients with type 2 diabetes who had a GPMP and TCA in the last 2 years, by jurisdiction, Indigenous primary health care organisations, December 2012, June 2013, December 2013, June 2014, December 2014 and May 2015
Source: AIHW analysis of national Key Performance Indicators for Aboriginal and Torres Strait Islander primary health care data collection
Implications
As discussed in relation to measure 3.05, organised chronic disease management in Aboriginal and Torres Strait Islander primary health care services has been demonstrated to result in improvement in various health outcomes (Hoy, W et al, 2000; Hoy, W et al, 1999; Rowley et al, 2000; McDermott et al, 2003; Bailie, R et al, 2007). Working with clients and their families to support proactive management of health conditions is vital (Griew et al, 2007).
A study of general practice patients with Type 2 diabetes found that, following implementation of care plans, the proportion of patients involved in multidisciplinary care and in the adherence to diabetes care guidelines increased. There were also improvements in patient metabolic control and cardiovascular risk factors (Zwar et al, 2007). Another study found an association between completing an annual cycle of care with good glycaemic control among diabetic patients (Esterman et al, 2016).
Barriers/enablers of chronic condition management strategies include: access to appropriate and affordable health services; effective clinical information management systems; coordination and TCAs; peer support; staff capacity and training in chronic condition management; engagement with clients and community; encouragement and support for clients; client knowledge of chronic conditions and their management; commitment to lifestyle change and family/peer support (Kowanko et al, 2012).
Negative experiences with specialists (e.g. discrimination, feeling patronised, judged and blamed) have influenced participants’ decisions not to follow up on doctor referrals, with these having negative implications for continuity and coordination of care (Aspin et al, 2012).
A range of government initiatives to tackle chronic disease and provide coordinated, effective care planning are covered in detail in the Policies and Strategies section.
The Australian Government provides funding through the Practice Incentives Program—Indigenous Health Incentive, to support general practices and Indigenous health services to provide better health care for Aboriginal and Torres Strait Islander patients, including best practice management of chronic disease.